






On January 7, 2021, at 0122 local (central standard -6 UTC) time, the bulk carrier Ocean Princess, with a crew of 24, struck the uncrewed/out-of-service oil and gas production platform SP-83A while operating in the Gulf of Mexico, 24 miles south of Pilottown, Louisiana (all mileage is given in nautical miles). No pollution or injuries were reported. Damage to the vessel and platform was estimated at $1.5 million.
BACKGROUND
The Ocean Princess was a dry bulk carrier built by Tsuneishi Shipbuilding of Fukuyama, Japan, in 2002 for Ocean Line Holdings of Qingdao, China, the beneficial owner of 32 vessels. The vessel was one of 32 managed by Ocean Longevity Shipping & Management Co. in Hong Kong, China.
Built in 1990, SP-83A was a US fixed oil and gas production platform located 11 miles offshore of Southwest Pass, Louisiana and 24 miles south of Pilottown, Louisiana, in the Gulf of Mexico, on the southern edge of the safety fairway that connected the approaches to Southwest Pass and South Pass to the Mississippi River. A four-pile steel structure in 467 feet of water that rose 73 feet above the water, the platform was 162 feet long and 81 feet wide and had three decks and a heliport. SP-83A was painted orange and equipped with eight flashing white lights with 2-mile visibility 53 feet above the water, and a fog signal with a two-mile range. It had been uncrewed since 2020, when it was taken out of service. SP-83A was owned by Arena Energy and managed by Arena Offshore of The Woodlands, Texas.
EVENT SEQUENCE
On December 28, 2020, the Ocean Princess arrived at the Harmony Street Wharf in New Orleans, Louisiana, with a cargo of steel and magnesium ore. According to the master, the plan was to discharge cargo for several days and then transit to the Gulf of Mexico, drift overnight, and return to New Orleans to load a cargo of grain. While drifting overnight, crew members would clean the cargo holds to prepare for the grain.
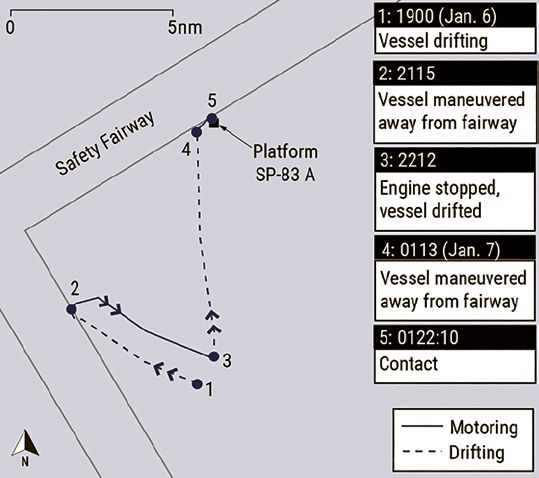
On January 6, 2021, after completing cargo discharge, the Ocean Princess got under way at 0722 with a pilot from the Crescent River Port Pilots’ Association at the conn (operational control of the vessel). After about a 6-hour transit downriver, an Associated Branch pilot boarded the vessel and assumed the conn from the Crescent River Pilot, who then departed the vessel via pilot launch. At 1506 the Associated Branch pilot departed the vessel at the pilot station, and the master assumed the conn as he directed the vessel during its transit to an area where the vessel would drift overnight, arriving about 1630. The engine was stopped, the master turned over the conn to the mate on watch (the chief officer), the engineering watch was instructed to have the engine ready for maneuvering within 15 minutes, and the master then left the bridge to rest.
The area where the vessel drifted bordered safety fairways to the north and west. There were three platforms in the drift area: two about 11 miles east-southeast of the intersection of the safety fairways, and SP-83A to the north. According to the master’s written night orders, the plan was to drift throughout the night with the engine on 15-minute standby, keeping clear of traffic and platforms. The night orders directed that, when approaching traffic or platforms, the mate on watch should call the engine room to make the engine ready to answer all bells and maneuver the vessel as necessary to avoid them. The crew had stopped cleaning cargo holds about 2000, and they would resume cleaning in the morning, then return to New Orleans as planned to load grain.
To give the crew members rest time after cleaning cargo holds during the day, the master scheduled himself to be on the bridge with the mate on watch, supplementing the watch and the duties of the lookout, from 2000 January 6 to 0400 January 7. The vessel had been drifting to the northwest since 1630 when, about 2108, the mate on watch called the engine room to ready the engine. Shortly thereafter (it took about 7 minutes to prepare the engine room) the vessel motored away from the western fairway with the master at the conn. At 2212, the engine was stopped, and the vessel again began to drift. According to the master, visibility was variable (2-3 miles in heavy rain and 5-6 miles in light rain).

indicated by a red X.
(Background source: Google Maps)
At 2355, the second officer relieved the third officer as the mate on watch, with the vessel drifting to the north in alternating heavy and light rain showers. The master and the second officer used the S-band/10-cm radar and the electronic chart display and information system (ECDIS) for contact detection. The X-band/3-cm radar was energized but in standby mode. The second officer said he was focused on short-range contacts and may have reduced the radar’s range from the 3-mile range to the 1.5-mile range.
The second officer logged the midnight GPS position and plotted a fix on the paper navigation chart. From 0014 to 0033, the master and the second officer reviewed stability calculations for the loading plan. At 0025, the vessel’s simplified voyage data recorder (S-VDR) documented the vessel’s heading as 042°, and the second officer informed the master that the vessel was drifting north at 357°. (An S-VDR is required to record fewer parameters— compared to a VDR—related to command and control of a vessel in addition to basic ship data. The vessel’s radar image was not recorded by the S-VDR, and it was not required because the S-VDR recorded automatic identification system data.)
The second officer took another fix about 0030. The fixes showed the Ocean Princess was drifting northerly at 2.4 knots. From 0033 to 0046, the master and chief officer, who had been summoned to the bridge by the master, discussed the stability calculations, and then the chief officer left the bridge. At 0048, the second officer reported that the vessel was 1 mile from the northern fairway. From 0051 to 0054, the master made a phone call to the company office.

from 1900 until the time of the casualty.
From about 0055 until 0120, about a minute before the casualty, the S-VDR captured the master engaged in a mostly one-sided conversation about non-navigational, non-pertinent matters with the second officer.
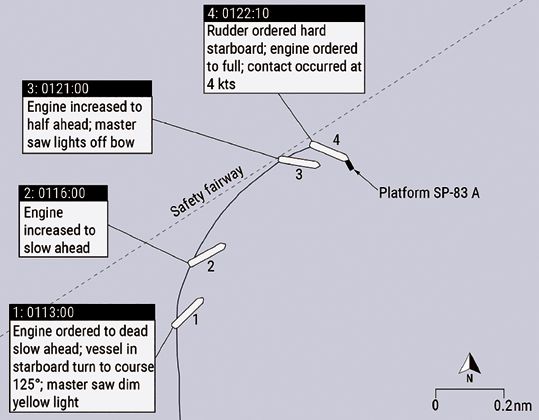
About 0100, the second officer informed the master that the vessel was approaching the safety fairway and then called the engine room to prepare for maneuvering. The second officer did not plot a 0100 fix on the paper chart but logged the vessel’s position in the GPS logbook. About 10 minutes later, the master took the conn. The second officer was on the engine order telegraph, and the master was operating the helm. According to the vessel’s S-VDR data, about 0112 the rudder moved to 30° starboard. At 0113, the master ordered the engine to dead slow ahead; the master said he was coming to a course of 125° to steer clear of the fairway. At the same time, the master stated he saw a dim yellow light, so he checked the radar. Not seeing any contacts, he checked the ECDIS and thought the light was from an oil platform 5-6 miles away, roughly on the same bearing. The second officer used binoculars to investigate and saw a light, but he could not tell how far it was from the vessel. The second officer later told investigators that he did not check the radar after seeing the light; he looked at the ECDIS and thought the light was a contact 5 miles away. The S-VDR captured the master asking, “Is that a ship?” The second officer responded, “Should be a platform.” At 0116, the engine was increased to slow ahead.
At 0121, the engine was increased to half ahead. At 0121:25, the S-VDR captured the master stating, “It’s getting closer.” The master later told investigators that when he saw multiple flashing lights, he realized there was something close to the vessel off the bow. The master ran out to the starboard bridgewing. At 0122:00, the master ordered the rudder hard to starboard and the engine full ahead. At 0122:10, the Ocean Princess’s starboard bow struck platform SP-83A at 4 knots speed over ground. The S-VDR captured the master saying, “Had a collision” at 0122:23.
The master ordered the rudder midships, stopped the engine, and sounded the emergency alarm. He told the chief officer via handheld radio to go to the bow and sound the tanks for flooding. After energizing a floodlight and pointing it forward, at 0127, the crew identified the object struck by the Ocean Princess as a platform (SP-83A). From 0128 to 0232, using various rudder orders and speeds, the master tried to steer away from SP-83A, but the vessel instead swung around the platform. When the vessel struck the platform, the anchor flukes and the anchor windlass were both affected. The starboard anchor became caught in the platform upon contact. Because the starboard anchor was on the brake rather than secured for sea, once it became entangled with the platform, the chain was pulled out as the vessel attempted to maneuver away from the platform.
The master told investigators that he could not move the vessel away from SP-83A and realized the starboard anchor chain was tangled in the platform’s structure. At 0232, the master ordered engine speed to dead slow astern to keep the vessel away from the platform. At 0250, the US Coast Guard Sector New Orleans Command Center was notified of the casualty by the vessel’s oil spill removal organization. Once daylight arrived, the master ordered the crew to cut the starboard anchor chain. At 0756, the starboard anchor chain was cut, casting off the anchor and 10.75 shots of chain. The vessel then transited to the Southwest Pass Fairway Anchorage to assess the damage and wait on further instructions from the company. On January 8, the Ocean Princess transited to New Orleans and moored.
Damage
The Ocean Princess sustained damage to the starboard bow, including starboard-side handrails, the starboard anchor windlass, and the bulwark. The forward mast was knocked down. There was also damage to portside handrails. Damage to the vessel was estimated to be over $500,000.
Platform SP-83A sustained damage to ladders, walk ways, and vent piping on three of four sides. Damage to the platform was estimated to be over $1 million.
Personnel
Postcasualty samples for toxicity tests were taken from all four deck officers and two crew members. All results were negative for alcohol and other drugs.
The master of the Ocean Princess had 31 years of experience at sea and 16 years of experience as a master. He had sailed to New Orleans at least four times, with his most recent port call before the casualty in July 2020. He had anchored in the Southwest Pass anchorage before but was not familiar with the area where the Ocean Princess was drifting at the time of the casualty; this was the first time he had attempted to drift near the southwest and south entrance passes to the Mississippi River in the Gulf of Mexico.
The second officer aboard the Ocean Princess had 10 years of experience at sea and had sailed with the company since 2011. He had previously sailed to New Orleans aboard the Ocean Princess in November 2019 and July 2020. He had not previously drifted offshore near the Mississippi River passes in the Gulf of Mexico.
The Ocean Princess tracked the amount of work and rest time for crew in accordance with the Standards of Training Certification and Watchkeeping for Seafarers (STCW) Code (2010). The STCW Code required watchstanders to receive a minimum of 10 hours of rest in any 24-hour period and that “hours of rest may be divided into no more than two periods, one of which shall be at least 6 hours in length.” The master reported working on January 6 from 0600 to 1600 with a 30-minute break from 1200 to 1230. However, according to the deck log, the master was on the bridge conning the vessel at 1600, and the deck log did not indicate if the mate on watch took the conn before 1630, when the crew first stopped the engine and the Ocean Princess started to drift. After being relieved about 1630, the master’s rest period was less than 4 hours before he assumed watch in lieu of the lookouts from 2000 until the time of the contact. The work-rest history for the second officer showed that he received 13 hours of rest in the 24-hour period before the casualty.
Detection of Platform SP-83A
The Ocean Princess management company’s safety management system (SMS) directed watchstanders to ensure safe navigation through a number of measures, including keeping a proper lookout and fixing ship position frequently, being familiar with the functions and limitations of navigation aids and instruments and using them correctly, and taking measures to keep clear of dangerous areas. According to the SMS, “Shoals, submerged reefs and obstacles on sea charts should be marked with red pencil for alert.”

source: Bureau of Safety and Environmental Enforcement)
As part of his normal routine while on watch, the second officer said he was looking out the bridge windows, using the S-band radar, checking the ECDIS, and plotting fixes on the paper chart every half hour beginning at midnight. He said he was aware of SP-83A from the paper chart but did not think it was of concern when he plotted his 0030 fix. He stated that he did not discuss the platform with the master but assumed the master was aware of it. The master said he was looking out the bridge windows, using the S-band radar and the ECDIS, and he knew that the second officer was plotting fixes on the paper navigation chart.
In their interviews, the master and the second officer said they never saw SP-83A on the radar. The second officer said the S-band radar was in good working condition and always kept in automatic tuned mode.
Navigation Charts
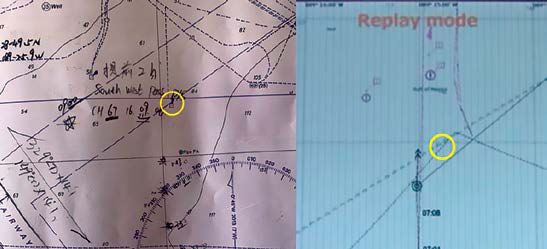
After the casualty, the master and the second officer noted that platform SP-83A was on the paper chart used on the bridge by the mate on watch, but SP-83A did not appear on the ECDIS. The second officer stated that during the time leading up to the casualty he did not notice SP-83A was missing on the ECDIS. The paper chart used on the bridge was British Admiralty chart 3857, Southern Approaches to the Mississippi River, 5th edition, December 20, 2012. The chart was up to date and corrected with the most recent British Admiralty weekly notice to mariners.
In the casualty location, the ECDIS drew its electronic navigation chart (ENC) information from the National Oceanic and Atmospheric Administration (NOAA) Nautical Information System (NIS) database. When reviewing the vessel’s ECDIS correction record for the previous year, investigators found that the automatic updates to the electronic navigation charts were received and loaded weekly to both ECDIS units aboard the Ocean Princess. The last update before the casualty was 53/21 (January 1, 2021). Neither of the two applicable NOAA ENC vector charts covering the area where the casualty occurred contained platform SP-83A. Although the Ocean Princess ECDIS unit was up to date with chart corrections, the two ENC vector chart updates did not contain platform SP- 83A, and therefore SP-83A was not shown on the Ocean Princess ECDIS unit.
Investigators also reviewed the three applicable NOAA paper navigation charts (11360, 11361, and 11366), which were up to date with the most recent notice to mariners, for the area where the casualty occurred. SP-83A was depicted on only chart 11360 but not the other two larger-scale charts. A representative of NOAA’s Marine Chart Division stated that platform SP-83A was added via a local notice to mariners in 1990, and the platform’s most recent revision was in 1994. For unknown reasons, SP-83A disappeared from charts 11361 and 11366 in March 2010. According to NOAA, ENCs were created from the raster (paper) charts, so the unexplained removal of platform SP-83A from the raster charts was critical to it also not appearing on the ENCs.
Since 2017, all NOAA ENCs have been stored in the NIS chart database and are no longer created from raster charts. Changes to an ENC must be made through the NIS database, and critical chart corrections are issued via the Coast Guard’s local notices to mariners. NOAA believes that, with NIS and its existing review procedure for ENC corrections and updates before public release, the error of SP-83A being omitted from ENC charts could not happen today.
Postcasualty Actions
After the casualty, Coast Guard District 8 (CGD08) issued a Broadcast Notice to Mariners via VHF radio from January 26 to February 9, which provided platform SP-83A’s position and notified mariners that the platform was not displayed on electronic charts. On February 3, CGD08 issued weekly Local Notice to Mariners 05/21 with the chart correction to add “Platform (Arena Offshore-107-1)” to the two large-scale paper NOAA charts covering the area where the casualty occurred. On February 11, NOAA released the automatic corrections that added platform SP-83A to the two ENC vector charts covering the casualty area.
ANALYSIS
Fatigue
The STCW Code requires watchstanders to receive a minimum of 10 hours of rest in any 24-period and that “hours of rest may be divided into no more than two periods, one of which shall be at least 6 hours in length.” Investigators found that the second officer met STCW work-rest requirements during the period before the casualty. During the 24-hour period (0001 to 2359) on January 6, the master had 13.5 hours of work and 10.5 hours of rest. The master reported working on January 6 from 0600–1600 with a 30-minute break from 1200–1230. He was conning the vessel at 1600.
After being relieved about 1630 when the vessel began drifting, he had a rest period of about 3.5 hours before assuming the watch from 2000 until the time of contact. It is likely that the master received less than 3.5 hours of sleep in the nearly 20 hours on board the Ocean Princess before the contact. The extended work hours and shortened off-watch hours from covering the lookout watch at 2000 put the master outside of the STCW work/rest limitations and left him susceptible to the effects of acute fatigue. Impacts of fatigue include difficulty concentrating, decreased ability to multi-task, increased risk tolerance, and reduced vigilance.
The effects of fatigue likely impacted the master’s performance in simultaneous roles as master and lookout, affecting his judgment and situational awareness in the events before the contact.
Distraction
In addition to watchstanding duties, the master was performing other tasks while on the bridge. Before the casualty, the master was recorded on the S-VDR spending 40 minutes reviewing stability calculations for the loading plan with the mate on watch (second officer) and then the chief officer before making a phone call to the company office. Next, from about 0055 until 0120, about a minute before the casualty, the master engaged in a mostly one-sided conversation about non-navigational, non-pertinent matters with the second officer.
Competing tasks, such as critical stability calculations, and personal conversations in the period leading to the contact likely distracted both the master and the second officer from their primary navigation duties. Distraction can reduce operator vigilance and negatively affect situational awareness.
Chart Error
Platform SP-83A was not charted on the official US electronic or paper navigation charts that provided the chart data to the ECDIS aboard the Ocean Princess, but the platform did appear on the British Admiralty paper chart that the mate on watch was using at the time of the casualty. The platform had been added to the US paper charts when installed in 1990, but for an unknown reason was omitted 20 years later in 2010 and remained off the two larger- scale US paper charts (charts 11361 and 11366) and ENCs for over 11 years—until after the casualty. Following the casualty, NOAA updated and corrected electronic and paper charts that had been erroneously missing platform SP-83A. Because ENCs have been stored in the NIS chart database since 2017 and the normal procedure for updating ENCs changed, NOAA believes the type of error that omitted SP-83A from the charts could not happen today.
Bridge Resource Management
Effective bridge resource management principles ensure the appropriate allocation and prioritization of tasks, use of available resources, effective communication among watchstanders, team collaboration, and maintenance of situational awareness. Despite the missing platform SP-83A on the ECDIS, the necessary information, equipment, charts, and personnel were available on board the Ocean Princess to safely operate the vessel. However, these resources were not used effectively.
Effective Communication and Team Collaboration
Upon departing New Orleans and exiting the Mississippi River, the master, in an effort to rest his crew that had been cleaning cargo holds throughout the day, reconfigured the bridge watch so that he would be on the bridge as a member of the bridge team and perform the duties vacated by the resting crew members. After resting below from about 1630 to 2000, the master reported to the bridge, working alongside the third officer, who was the mate on watch. The master remained on the bridge with the second officer after he relieved the third officer as mate on watch about midnight.
The master’s night orders instructed the bridge team to drift throughout the night with the engine on 15-minute standby, keeping clear of traffic and platforms. The night orders directed that, when approaching traffic or platforms, the mate on watch should call the engine room to make the engine ready to answer all bells and maneuver the vessel as necessary. Instead of planning the drift route, identifying obstacles on the navigation charts (paper and electronic), and identifying or plotting out no-go areas ahead of time, the bridge team was left to adapt as they drifted along with the wind and current.
When the master arrived on the bridge for the watch starting at 2000, he effectively became part of the bridge team navigating the vessel, as opposed to a master overseeing the bridge team. According to interviews and statements, there was no clear delineation of duties between the mate on watch and master. When the master deemed it necessary to maneuver, he took the conn and gave engine and rudder orders.
The presence of the master on the bridge also could have impacted the behavior of the second officer as the mate on watch. Leading up to the point where the master took the conn, the mate on watch (the second officer) had operational control of the vessel. However, because of the master’s positional authority, superior knowledge, and experience, the master’s presence could have caused the mate on watch to make assumptions that he would not have made had the other bridge watchstander been another crew member. As an example, although he was aware of SP-83A from the paper chart, the second officer told investigators that he did not discuss platform SP-83A with the master, but rather had assumed the master was aware of it.
Use of Available Resources
Nine minutes before the casualty, with the master at the conn, the master and the second officer saw a light but did not recognize that the light was from platform SP-83A. The master checked the radar after observing the light but saw no contact. The master and second officer told investigators they checked the ECDIS, which did not show platform SP-83A, and thought that the light was from an oil platform about 5 miles away. The bridge officers took no additional steps to verify whether the light posed a risk to safe navigation.
There were three platforms in the general area where the vessel was drifting. Although platform SP-83A was depicted on the British Admiralty paper chart on the bridge, it was not marked as an obstacle with red pencil as required by the company’s SMS, nor were the other two platforms nearby. The second officer said he was aware of the platform when he plotted fixes on the paper chart nearly an hour before the casualty but did not think it was of concern. He also stated that he did not tell the master about the platform on the chart and assumed the master was aware of it.
The bridge officers never identified platform SP- 83A on the radar. In varying conditions of visibility, they used only one of two radars available, the S-band/10-cm radar. The X-band/3-cm radar, which was energized and available, was kept in standby. With only the S-band radar in use, the bridge team’s detection of traffic or other navigation obstructions was limited by the range selected by the bridge officers (in this case, either 1.5 or 3 miles) and accuracy of this radar’s display.
When making assessments or predictions about a situation, there can be a tendency to rely more heavily on information that reinforces one’s expectations and discount or avoid information that may contradict those expectations. In this case, both the master and the second officer told investigators that they saw the lights of the platform they eventually struck but were under a belief, or bias, that SP-83A was farther away because it did not appear on the radar or the ECDIS. Operating under this belief, the bridge team did not seek out information through alternative navigation resources to either confirm or deny their bias. Furthermore, despite identifying SP-83A on the paper chart, the mate on watch discounted this information and did not communicate it with the master. This concept is called confirmation bias. When the bridge team saw multiple lights 1 minute before the casualty, they realized a contact was close to the vessel. They did not identify that the object they struck was a stationary platform until a few minutes after contact.
Thus, there were missed opportunities for the bridge team to correctly identify the presence of platform SP-83A and assess it as a risk to navigation before the casualty. The officers did not effectively assess the risk or cross-check with other navigation tools to investigate the lights further.
CONCLUSIONS
The National Transportation Safety Board determines that the probable cause of the contact of the dry bulk carrier Ocean Princess with the oil and gas production platform SP-83A was poor bridge resource management, which resulted in the bridge team not identifying the platform and recognizing the risk it posed to their safe navigation even though they saw its lights about 10 minutes before the casualty. Contributing was platform SP-83A not being shown on the vessel’s electronic chart display and information system due to a charting error.
LESSONS LEARNED
The effective use of all available resources by a bridge team, including paper charts, electronic charts, and radars, increases collective situational awareness and contributes to a safe navigation watch.
When identifying hazards, bridge teams should avoid over-reliance on a single data source by cross-checking information with available bridge resources and communicating identified risks with fellow watchstanders to ensure a shared mental model.
Increasing operator vigilance and combating over-reliance requires healthy skepticism about situations and information sources regardless of how accurate they could be, or how confident one is in their own assessment. In this casualty, the electronic chart display and information system (ECDIS) was missing the oil platform struck by the vessel due to a charting error. The vessel’s safety management system noted, “ECDIS is a valuable asset in assisting navigators and allowing them more time to maintain a proper lookout by providing them with more detailed situational awareness.” However, it also warned, “navigators should always cross check ECDIS information with the other sources,” and, if not used properly, “ECDIS may contribute to accidents rather than preventing them.” The inability to recognize the fallibility of technology, such as an ECDIS, can result in operator over-reliance and overconfidence that degrades sound navigation practices and negatively affects situational awareness.
Republished from Marine Construction Magazine Issue V, 2022


